You're losing muscle right now. Here's why it matters more than you think.
Last month we talked about neurological overload, how stress fills your glass and what happens when it spills over. Understanding your neurological load is one of the most important things you can do for your health. This month's topic is just as valuable, and it's connected in ways most people don't realize.
We want to talk about muscle loss. Not to scare you or be negative about it. Your health is a responsibility that each of us has to undertake for ourselves, and we believe the more you understand about what's actually happening inside your body, the better equipped you are to do something about it. We're here to help guide you. That's all we've ever tried to do.
So. Muscle. Not because people aren't strong enough to open a jar. Because muscle is doing things inside your body that most people, and honestly most doctors, never talk about.
You've been losing muscle since your 30s
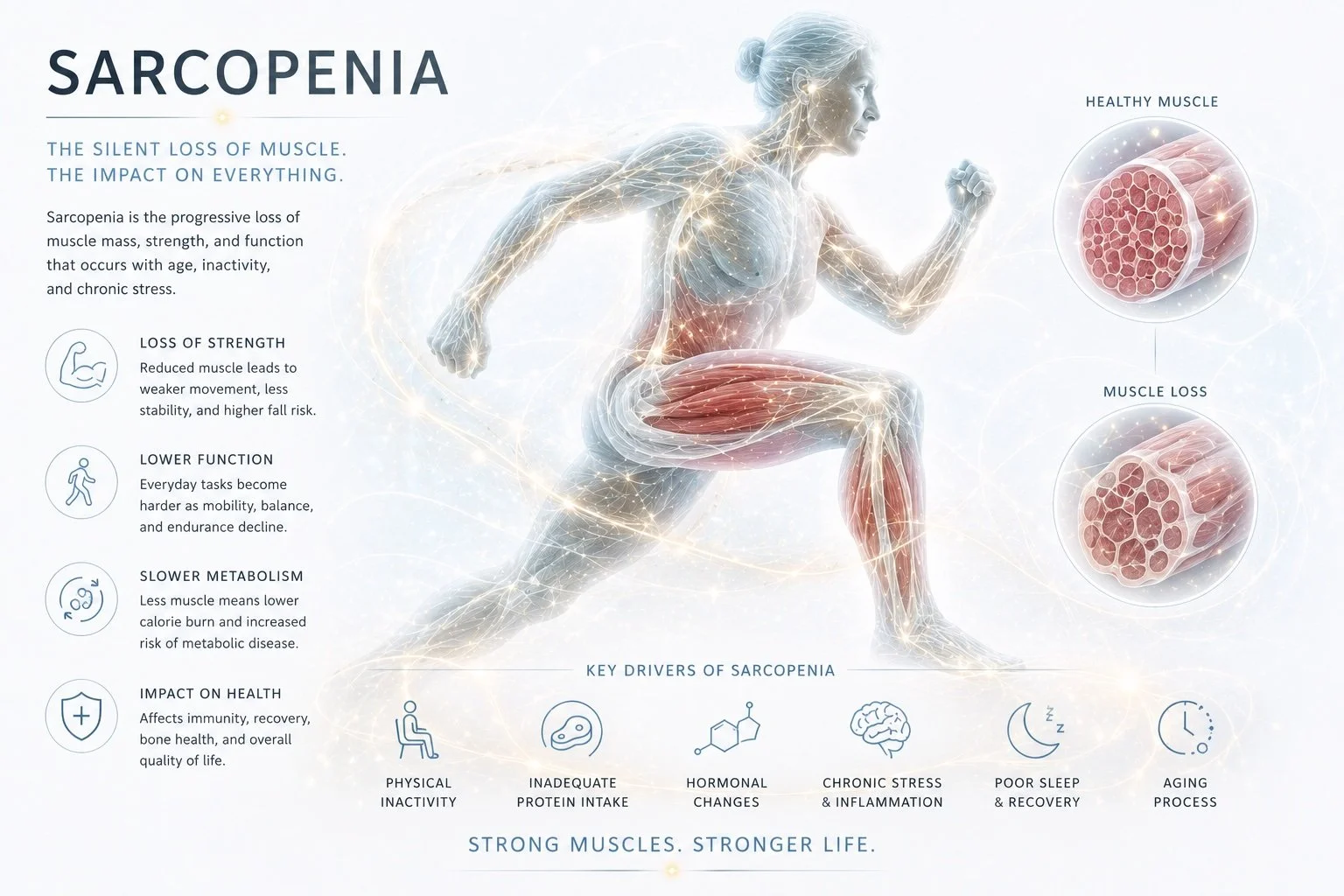
Starting around age 30, your body begins breaking down more muscle protein than it builds. The decline is slow at first, maybe 3-5% per decade. By 40, it accelerates. After 50, you can lose up to 1-2% of your muscle mass per year if you're not actively working against it.
For women, perimenopause is when the ground starts shifting. Estrogen is protective of muscle tissue, and as it starts to fluctuate and decline, your body's ability to build and hold onto muscle quietly drops with it. By menopause, it's not a slow leak anymore. It's an open faucet. For men, declining testosterone does the same thing on a slightly different timeline.
The medical term is sarcopenia. It literally means "poverty of flesh" in Greek. Most people have never heard of it, and their doctors have never mentioned it, even though it's one of the strongest predictors of how you'll age, whether you'll fall, how fast you'll recover from illness, and whether you'll be able to live independently in your 70s and 80s.
The GLP-1 problem nobody's talking about
While we're on the subject of muscle loss, we need to talk about what's happening right now with GLP-1 medications like Ozempic, Wegovy, and Mounjaro. Millions of Americans are taking these drugs for weight loss, and the weight is coming off. But so is their muscle.
A 2024 review in Diabetes, Obesity & Metabolism found that 15-60% of the weight lost on GLP-1 receptor agonists comes from lean mass, not fat. In the STEP 1 trial for semaglutide (Ozempic/Wegovy), 45.5% of the weight lost was lean mass. Nearly half. In the SURMOUNT-1 trial for tirzepatide (Mounjaro), about a third of the weight lost was lean mass.
An editorial in Annals of Internal Medicine warned that these drugs may be accelerating sarcopenia in older adults. And a 2026 study out of Stanford found that unlike fat, muscle doesn't come back quickly after GLP-1 use. Once it's gone, rebuilding it takes real work.
We're not saying these medications don't have legitimate uses. For some people, they're life-changing. But if you're on a GLP-1 and you're not doing resistance training alongside it, you're trading one problem for another. You're losing the organ system that protects you from chronic disease, and you may not realize it until the scale looks great but your body can't do what it used to.
If you're on one of these medications, everything in this blog applies to you even more urgently. Resistance training and adequate protein aren't optional add-ons. They're the only way to make sure the weight you're losing is the weight you actually want to lose.
Muscle is an organ, not decoration
Dr. Gabrielle Lyon is a board-certified physician who trained in geriatrics and nutritional science. Her 2023 book Forever Strong makes an argument we wish more people heard: "The problem isn't that you're over-fat. It's that you're under-muscled."
She's not being cute. Skeletal muscle is the largest endocrine organ in your body. It releases over 600 signaling molecules called myokines every time it contracts. Those molecules travel through your bloodstream and talk to your brain, your bones, your immune system, your liver. They reduce inflammation. They improve how your body handles glucose. Some of them have been shown to suppress tumor growth.
Muscle is also where most of your blood sugar goes after you eat. About 80% of glucose disposal happens in skeletal muscle. When you have less muscle, your body has fewer places to put that glucose, which means higher blood sugar, more insulin resistance, and eventually metabolic syndrome or type 2 diabetes. This is why people who strength train tend to have better metabolic panels than people who only do cardio, even at the same body weight.
When we tell clients that muscle is an organ of longevity, not a vanity project, you can see the shift in their face. It changes the conversation completely.
Inflammaging: the cycle you're probably already in
Remember the glass from last month, how every kind of stress pours into it? Muscle loss feeds a similar buildup, except this one happens at the cellular level.
As you lose muscle, your body produces fewer anti-inflammatory myokines and more pro-inflammatory signals. Researchers call this state "inflammaging," a word that does exactly what it sounds like. Chronic, low-grade inflammation that accelerates aging even when you're not sick, injured, or fighting an infection.
Inflammaging is connected to almost every condition we see in midlife clients. Joint pain that shows up without an injury. Slower recovery from workouts. Brain fog. Metabolic issues. Bone density loss. Autoimmune flare-ups. These don't happen in isolation. They share a common inflammatory driver, and muscle loss is feeding it.
The cycle goes like this: you lose muscle, inflammation goes up. Inflammation goes up, your body breaks down muscle faster. You lose more muscle, inflammation goes up further. It's a feedback loop, and it runs quietly in the background for years before you notice something's wrong.
Zombie cells
Part of what makes inflammaging so persistent is cellular senescence. As you age, some of your cells stop dividing but refuse to die. They just sit there, taking up space and leaking inflammatory molecules into the surrounding tissue. Researchers have started calling them zombie cells, and the name fits.
Everyone accumulates senescent cells over time. That's normal biology. But the rate accelerates when you're sedentary and losing muscle. The inflammatory signals these zombie cells pump out, things like IL-6 and TNF-alpha, are the same markers that show up in every inflammaging study. They're part of the reason your joints ache more than they used to, your recovery takes longer, and minor injuries seem to linger for weeks.
Resistance training has been shown to reduce the accumulation of senescent cells and lower the inflammatory signals they produce. Your muscles aren't just fighting sarcopenia when you train. They're helping your body clear out cellular debris that's been stoking the fire.
If you want to go deeper on senescent cells and the biology of aging, David Sinclair's Lifespan: Why We Age and Why We Don't Have To is a good starting point. He breaks down how zombie cells accumulate, why the cytokines they release cause a cascade effect (turning healthy cells senescent too), and why researchers are working on senolytic compounds that can clear them out. The science on cellular senescence has moved fast since the book came out in 2019, but the foundation he lays is still one of the most accessible explanations out there.
If you want to support this from the nutritional side, Designs for Health makes Senolytic Synergy, a blend of fisetin and quercetin (the two most-studied senolytic compounds) along with curcumin and Senactiv, formulated to help your body clear senescent cells and calm the inflammation they drive. Training is still the foundation, but it's a reasonable addition if this is an area you want to target directly. Use code MUSCLE15 at checkout for 15% off.
Your legs are protecting your brain
One study that stuck with us: researchers at King's College London followed 324 twins over 10 years (Steves et al., 2015, Gerontology). They measured leg strength at the start and then checked cognitive function and brain structure a decade later.
The twin with stronger legs had better cognitive function and more grey matter. Same DNA. Same childhood. Same family environment. The difference was leg strength.
Leg strength was a better predictor of brain health than any other lifestyle factor they measured. Not diet. Not cardiovascular fitness. Not education level. Leg power.
Your legs are your largest muscle group. When they're strong, they're producing more myokines, disposing of more glucose, and sending more protective signals to your brain than any other tissue in your body. When they're weak, all of that declines.
We bring this up with clients who tell us they skip leg day. It usually changes the conversation.
The problem with "just lift heavy"
All of this points to one thing: you need to be doing resistance training. The science is about as settled as it gets in exercise research.
If you follow any of the current conversation around women over 40 and resistance training, you've probably heard the message: lift heavy. Dr. Stacy Sims, an exercise physiologist whose research on women's hormonal physiology has changed the field, recommends heavy compound movements (squats, deadlifts, presses) at high intensity, 3-6 reps per set, to counteract the anabolic resistance that comes with declining estrogen. She's right. The research supports it. For women who are already training, who know their way around a squat rack, and who have the movement foundation to handle heavy loads safely, that advice is solid.
But that's not most people.
Most of the people we see at HPC aren't athletes. They're not coming from a training background. They're women (and men) who haven't exercised consistently in years, or decades. They've tried following a program from Instagram or YouTube, jumped into something their body wasn't prepared for, and wound up hurt within the first month. A tweaked back. A flared-up knee. A shoulder that won't calm down. So they stop. And the sarcopenia keeps rolling. The inflammaging keeps building. The zombie cells keep accumulating.
The gap in the conversation is massive. The science says resistance training is non-negotiable. The loudest voices say go heavy. But nobody is talking about the people who can't even get to the starting line without getting hurt. You can't load a movement pattern your body hasn't learned yet. You can't go heavy on a squat if your glutes aren't firing and your hip flexors are locked up from 20 years of sitting. That's not training. That's a countdown to injury.
How you start matters more than how heavy you go. The foundation has to come first.
Find out where you stand
In clinical settings, grip strength has been the gold standard for measuring sarcopenia risk for decades. It's one of the first things a geriatrician will test. The problem is that most people don't have access to a dynamometer, and they're not going to buy one to find out if they're losing muscle. That said, if you're the type who wants to test your grip directly, an inexpensive hand-grip dynamometer will give you a real number you can track over time.
That's why we built the Muscle and Longevity Assessment around the 30-second chair stand test instead. It's a validated clinical screening tool that measures lower body strength and endurance, and all you need is a chair and 30 seconds. Your results are compared against published norms for your age and sex, so you get a real number, not a guess.
The full assessment goes beyond the chair stand. It covers your training habits, functional strength, recovery markers, metabolic health, nutrition, mobility, and lifestyle factors across 30 questions. Takes about 5 minutes, your results are completely private, and nothing is stored or sent to us.
If the blog above made you wonder where you actually stand, this is the fastest way to find out.
Take the Muscle and Longevity Assessment
Where we go from here
This is why Kele built Movement by Design. Not because the "lift heavy" research is wrong. Because there's a step that comes before it that almost everyone skips.
"I built this course for people who want to feel better in their bodies, but don't know where to turn for help. It's designed for beginners to intermediate level of exercise experience. If you're wondering if this class would be a good fit for you, it probably is! I can't wait to see you all next month!"
Kele McDaniel
Movement by Design is a 4-week foundational movement course that teaches your body how to activate the right muscles in the right order before you add any real load. Glute activation, psoas engagement, hip mobility, core stability, breathing mechanics, functional movement patterns, upper body integration. All sequenced neurologically and anatomically so your body learns to move correctly first and load safely later. It's designed to give people the tools to start a movement routine safely and progress in a way your body is designed to adapt, not a way that breaks it.
After 25 years and over 40,000 hours of client work, Kele has seen the same pattern hundreds of times. Someone gets motivated by a podcast or a social media post, jumps into a program built for people who already have a foundation, and gets hurt. Not because the exercises were bad. Because their body wasn't ready for them. The muscles that were supposed to be doing the work weren't firing. The muscles that were supposed to be stabilizing were locked up or asleep. So the load went somewhere it shouldn't have, and something gave.
Movement by Design is the missing step. It's designed for women 40 and older, though the principles apply to anyone who feels like something in the way they move is off. One live class per week, video replays, a private group for questions, and a take-home routine you can use three times a week for as long as you want. $25 in resistance bands and no gym membership. Once you have the foundation, you can go as heavy as you want. But the foundation has to come first.
The beta is $47. Details are on the Movement by Design page.
If you're already training and want to support your muscles from the nutritional side, we wrote about a few supplements we recommend in this month's newsletter: Performance Peptides (fava bean peptides for muscle protein synthesis), Whole Body Collagen (collagen peptides for connective tissue and joints), and Creatine Monohydrate (muscle preservation, bone density, and cognitive function). All by Designs for Health. Use code MUSCLE15 at checkout for 15% off any of them.
And if you haven't tried our Flexibility for Optimal Aging routine yet, everything we wrote last month about neurological overload still applies. Stretching drains the glass. Resistance training makes sure you have the muscle to keep the glass from filling up so fast in the first place. They work together.
What the research says
We promised in the newsletter to link the specific studies, so here they are.
On muscle strength and sarcopenia: a 2025 meta-analysis of 12 randomized controlled trials found that resistance training improved muscle strength, gait speed, and physical function in older adults with sarcopenia. The gains were measurable within weeks of starting a program (Frontiers in Public Health).
On inflammation: a 2022 systematic review and meta-analysis of RCTs confirmed that resistance training reduces C-reactive protein and IL-6, two of the most commonly used markers of chronic inflammation, in older adults. A separate 2024 meta-analysis on ScienceDirect found similar results specifically for middle-aged and older adults.
On bone density: a 2025 meta-analysis of 17 RCTs showed that resistance training improves bone mineral density at the lumbar spine and femoral neck in postmenopausal women. The optimal protocol was high-intensity (70% or more of your one-rep max), three times per week (Journal of Orthopaedic Surgery and Research).
On metabolic health: a 2021 meta-analysis of 43 RCTs covering over 2,000 participants (56% women, average age 57.8) found that resistance training improved fasting glucose and insulin resistance markers.
Every study lands in the same place. If you're only going to do one type of exercise as you age, it should be resistance training. We don't say that lightly.
We've been telling clients for years to take care of their muscles. Now you know why.